
You notice a sore patch on your tongue, then a few white spots on the inside of your cheek. By that evening, food feels irritating, and you're searching to work out whether this is something minor, something contagious, or something that needs a script.
That pattern is common with oral thrush, also called oral candidiasis. It's a fungal overgrowth in the mouth, and while it can look alarming, it's usually very treatable. In practice, what unsettles people most isn't only the discomfort. It's the uncertainty. They want to know whether a lozenge will sort it out, whether they've caused it somehow, and when it stops being a simple problem.
Oral thrush also isn't limited to one age group or one life stage. I see it in adults with dry mouth, denture wearers, people using steroid inhalers, and occasionally in children as well. If you're reading because a child has symptoms, our guide to paediatric dental care may also help you think through when a dental review is sensible.
If thrush symptoms are tied to breastfeeding concerns, it can also be useful to understand the broader picture around nipple symptoms and cross-infection. Bornbir's guide to nipple thrush is a practical resource for that situation.
What Is Oral Thrush and How Can Lozenges Help
Oral thrush happens when Candida, a yeast that can live in the mouth without causing trouble, starts to overgrow. When that balance shifts, you may notice white patches, a red or burning feeling, soreness under dentures, cracks at the corners of the mouth, or a generally coated, uncomfortable mouth.
For many people, oral thrush lozenges are one of the first treatments discussed because they deliver antifungal medicine directly where the infection is sitting. That local action is the key point. These aren't throat sweets or soothing pastilles. They're medicated lozenges used to treat fungal infection on the oral tissues.
Why people often reach for lozenges first
A lozenge makes sense when the problem appears localised to the mouth and the person can comfortably let it dissolve as directed. It's practical, targeted, and familiar. In Australia, that usually means a clotrimazole troche rather than a broad systemic antifungal.
What I often need to clarify is that a lozenge is only helpful when the diagnosis is right. White patches in the mouth can have more than one cause. Trauma, ulceration, friction from dentures, dry mouth changes, and other oral conditions can all confuse the picture.
Practical rule: If you're not sure it's thrush, don't assume a lozenge is the answer just because the mouth looks white or feels raw.
The stigma around thrush is unnecessary
Patients sometimes feel embarrassed, as though oral thrush means poor hygiene. That's not how real life works. Thrush often appears because something has changed in the mouth's environment or the body's defences. Dentures, inhaled steroids, smoking, dry mouth, recent illness, or an underlying medical issue can all play a part.
The good news is that there's usually a sensible next step. Sometimes that's straightforward local treatment. Sometimes it's checking why the problem showed up in the first place.
Understanding How Oral Thrush Lozenges Work
In Australia, oral thrush lozenges are generally clotrimazole 10 mg troches, used as a local antifungal treatment for oral and oropharyngeal candidiasis. The standard regimen across major drug references is 1 lozenge dissolved slowly in the mouth five times daily for 14 days, while prevention regimens are commonly 3 times daily in people at increased risk. Australian consumer guidance also states they're intended for adults and children aged 3 years and older (GoodRx overview of clotrimazole troches).
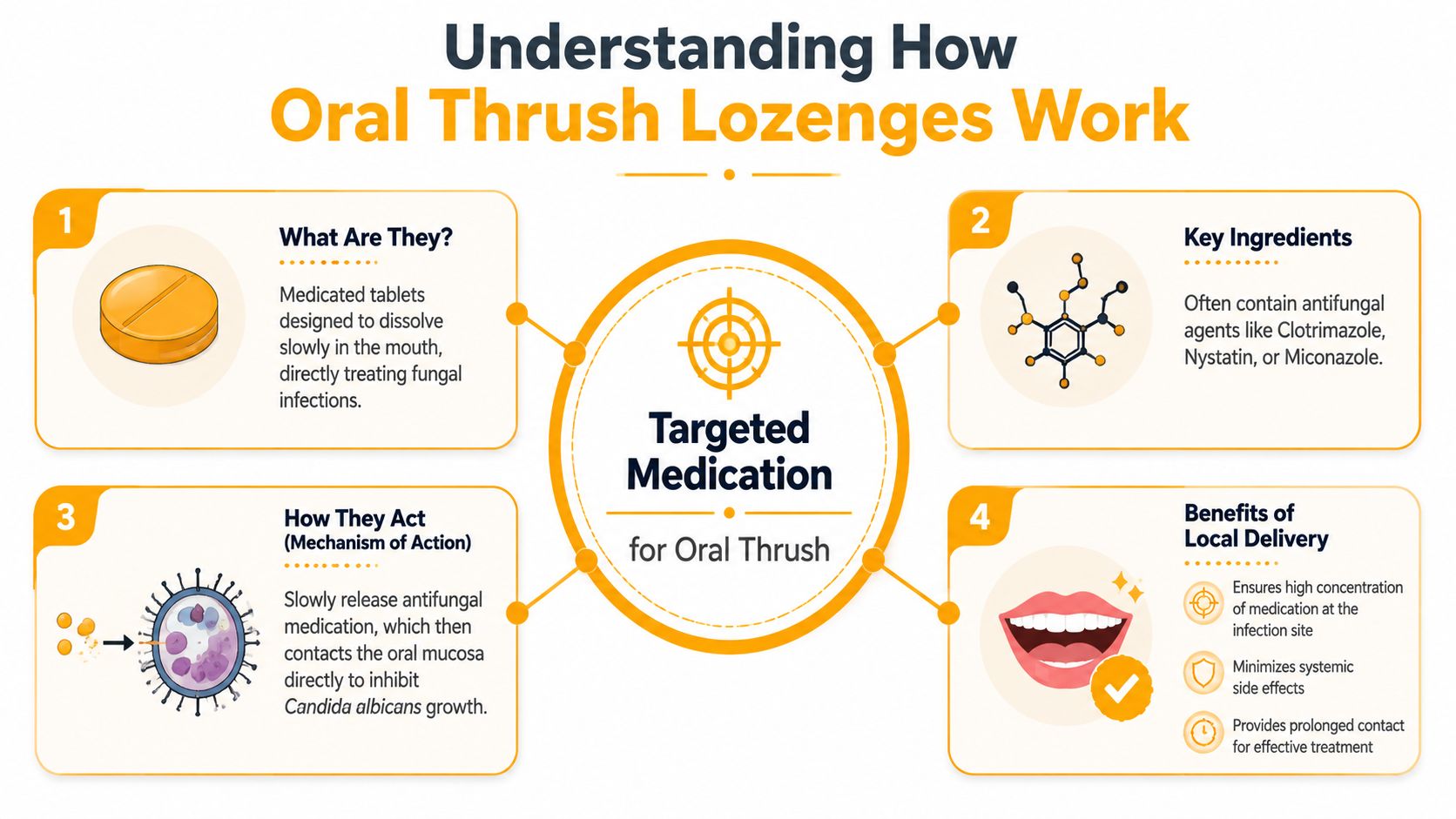
Local treatment, not a general mouth remedy
A good way to think about the lozenge is as a careful delivery system. If thrush is like weeds growing across the surface of a garden bed, the lozenge places the antifungal exactly where those weeds are growing. It doesn't work best by being swallowed quickly. It works by staying in contact with the lining of the mouth.
That's why these lozenges are described as local therapy. The medicine is meant to act on the oral tissues and the fungal colonies sitting there. For a patient with straightforward oral thrush, that local approach is often the whole point.
Why the slow dissolve matters
People are sometimes surprised by how specific the instructions are. That's because the benefit depends on contact time. A lozenge that melts gradually coats the mouth for longer, which gives the antifungal a better chance to act.
That also explains why they can feel more effortful than a tablet. You can't treat them like a standard pill and expect the same effect. If someone knows they're unlikely to manage that routine well, another topical format may be easier.
For readers comparing other products used for sore mouths, this guide to the best mouth ulcer gel in Australia can help clarify the difference between treatments for ulcers and treatments for fungal infection. They aren't interchangeable.
The lozenge only works properly if it behaves like a lozenge, not like a swallowed tablet.
Who lozenges suit best
Lozenges tend to suit people who can:
- Follow the timing well and space doses through the day
- Allow a slow dissolve without chewing
- Tolerate a medicated taste or mouth feel
- Use them safely, especially if they're old enough to manage the lozenge appropriately
They're often less convenient for very busy adults, people with significant dry mouth, and patients who want something faster than the lozenge format can realistically provide.
Correct and Safe Use of Antifungal Lozenges
Used well, oral thrush lozenges can be very effective. Used badly, they underperform. The difference usually comes down to technique.

Clotrimazole lozenges should be allowed to dissolve in the mouth over 15 to 30 minutes, and patients should not chew them, swallow them whole, or eat or drink during administration. Safety labelling also reports unpleasant mouth sensations, nausea or vomiting, and abnormal liver-function tests, with one source noting increased SGOT in about 15% of trial patients (Mayo Clinic guidance on oral clotrimazole).
How to take them properly
Most problems I see with lozenges are practical ones rather than medical ones. People are in a rush, they chew them, they have coffee straight after, or they stop as soon as the mouth feels a bit better.
The basics are simple:
- Place the lozenge in the mouth and let it dissolve slowly.
- Move it around gently if needed so the medication contacts different areas.
- Don't chew or crush it. That shortens contact time.
- Don't swallow it whole. That defeats the local treatment effect.
- Avoid eating or drinking while it dissolves. You don't want to wash the medication away.
What tends to go wrong
A few patterns come up again and again:
- Rushing the dose. If the lozenge disappears too quickly, the mouth hasn't had enough medicated contact.
- Using it like a sweet. Constant biting or sucking aggressively can reduce how evenly it works.
- Stopping early. Symptoms may settle before the fungal overgrowth has fully cleared.
- Ignoring oral triggers. If dentures aren't cleaned properly or inhalers aren't followed with rinsing, the environment that encouraged thrush may still be there.
Good prevention habits make any treatment plan more effective. If you want to tighten up your routine more broadly, our article on preventive dental care is a helpful place to start.
Here's a practical demonstration of oral care technique that may help some patients think about medication use and mouth management more carefully:
Side effects and sensible caution
Short-course local treatment is reasonably well-tolerated, but it's still medication. An odd taste, mouth irritation, or nausea can happen. The liver test finding is worth knowing about, not because patients should panic, but because it reinforces an important principle. These lozenges are best used thoughtfully and for the intended course rather than casually repeated without review.
If a treatment only works when used correctly, technique isn't a minor detail. It's part of the treatment.
When Lozenges Are Not Enough
The biggest mistake people make with oral thrush lozenges is assuming they're a cure-all. They're not. They're a local treatment for a local problem, and once the pattern becomes persistent, recurrent, or medically complicated, the conversation changes.
Drug references note that lozenges are for local treatment and may not be right for everyone. Recurrent or high-risk cases, including those in denture wearers or people with diabetes, may need professional investigation for underlying causes rather than just another course. The National Study of Adult Oral Health found roughly 1 in 5 Australian adults had diabetes, a known thrush risk factor (DailyMed-related summary of local treatment limits and risk context).
Situations where a lozenge may be the wrong tool
A lozenge may not be enough if:
- The patches keep coming back after treatment
- You wear dentures and the tissues underneath stay sore
- You use a steroid inhaler and symptoms repeat
- You have diabetes or another health issue that can alter healing or increase fungal overgrowth risk
- The appearance is unusual or doesn't behave like typical thrush
- The soreness is worsening rather than settling
These cases need more than a repeat script. They need an assessment of what's driving the problem.
Why recurrent thrush deserves a closer look
When I see recurrent oral soreness, I don't only ask what medication was used. I ask what else is going on in the mouth and in the person's health. Denture fit, dry mouth, oral hygiene technique, inhaler use, smoking, and medical history can all matter.
That's why blindly repeating local antifungals can become unhelpful. If the environment hasn't changed, the mouth may keep drifting back to the same problem. If the diagnosis is wrong, the lozenge may never have been the answer.
For adults who haven't had an oral examination in a while, a check-up and clean is often where these patterns get picked up properly. It's less about “getting teeth cleaned” and more about looking at the whole mouth with fresh eyes.
Persistent thrush is often a clue. Good care means asking what the clue is pointing to.
When to stop self-managing
Self-care is reasonable when symptoms are mild, clearly fit with thrush, and improve as expected. It stops being reasonable when symptoms linger, repeat, or sit alongside risk factors that make the situation more complicated.
At that point, the goal isn't to be alarmist. It's to be accurate.
Alternatives and Complementary Dental Care
Lozenges are only one tool. In practice, some patients do better with another topical treatment, and some need a broader plan that tackles the oral environment as well as the fungus.
While transient liver enzyme elevations have been reported in up to 15% of patients using oral clotrimazole, clinically significant liver injury hasn't been linked. That supports its use, but it also highlights the value of prevention, especially for denture wearers, inhaled corticosteroid users, and smokers, who are advised to reduce risk through measures such as cleaning dentures, rinsing after inhalers, and limiting sugar intake (LiverTox summary on oral clotrimazole and prevention context).
Oral thrush treatment options at a glance
| Treatment | Best For | How It Works | Considerations |
|---|---|---|---|
| Clotrimazole lozenges | Localised oral thrush in patients who can manage slow-dissolve dosing | Delivers antifungal medication directly across oral tissues | Technique matters. Less convenient if you're rushing, very dry-mouthed, or dislike lozenges |
| Antifungal gel | Patients who need a topical option that can be applied directly | Coats affected areas with antifungal medication | Can be easier for some mouths, but still needs proper application |
| Antifungal mouth rinse or suspension | People who benefit from broader coating through the mouth | Contacts oral tissues through swishing | Useful in some situations, but compliance and timing still matter |
| Systemic antifungal tablets | More persistent, extensive, or medically complicated cases | Treats beyond a strictly local surface level | Usually needs professional diagnosis and prescription |
| Supportive oral care | Anyone with thrush risk factors | Reduces the conditions that allow Candida to persist | Helps treatment work better, but doesn't replace antifungal therapy when infection is active |
The overlooked part of treatment
Medication gets the attention, but the mouth's daily environment often determines whether the problem settles or keeps returning.
Focus on the basics:
- Clean dentures thoroughly and don't leave them in constantly if you've been advised to remove them
- Rinse after steroid inhalers so medication residue doesn't sit in the mouth
- Address dry mouth rather than accepting it as normal
- Cut back on frequent sugar exposure if it's become a habit
- Review smoking as part of oral health, not as a separate issue
Matching the treatment to the patient
A lozenge can be excellent for one patient and awkward for another. Someone with excellent routine, mild local thrush, and no major risk factors may do very well. Someone with repeated episodes under a denture, ongoing dry mouth, or a more complicated medical background may need a different route entirely.
That's where dental judgement matters. The right treatment isn't the one that sounds strongest. It's the one that fits the actual cause and the way the patient can realistically use it.
Preventing Oral Thrush and When to Visit The Smile Spot
Prevention works best when it's practical enough to keep doing. If you've had thrush before, the aim isn't to sterilise the mouth. It's to make the mouth a less favourable place for fungal overgrowth.
A definitive diagnosis should ideally be confirmed by KOH smear and/or culture before treatment. In immunocompromised patients, lozenges may also be used prophylactically at one lozenge three times daily during periods of risk, which underlines the importance of a professionally managed prevention strategy (DailyMed consumer information on diagnosis and prophylaxis).
A sensible prevention checklist
- Keep dentures clean and have them reviewed if they're rubbing or trapping debris
- Rinse after inhalers every time if you use inhaled corticosteroids
- Pay attention to dry mouth because persistently reduced saliva changes the balance in the mouth
- Don't ignore repeat episodes just because they responded once before
- Book regular dental care so tissue changes are assessed properly, not guessed at
For households trying to keep everyone's oral health on track, our article on family dental care may help you think about prevention as an everyday routine rather than a reaction to symptoms.
When to book instead of waiting
A dental visit is the right next step if the diagnosis isn't clear, the problem keeps returning, the mouth is becoming more painful, or you have risk factors that make a simple repeat course less reliable.
You also shouldn't feel judged for coming in early. That's often the best time to sort it out. A careful oral examination can help confirm whether this is thrush, whether another condition is mimicking it, and whether there's a reason your mouth has become more vulnerable.
Early review is often simpler than repeated self-treatment that never quite fixes the problem.
If you're dealing with oral soreness, white patches, recurring thrush, or denture-related irritation, The Smile Spot can help you get a clear diagnosis and practical treatment plan. Our Dulwich Hill team provides gentle, family-focused dental care for patients across the Inner West, with personalised advice that looks beyond the prescription and addresses what's driving the problem.






")















































